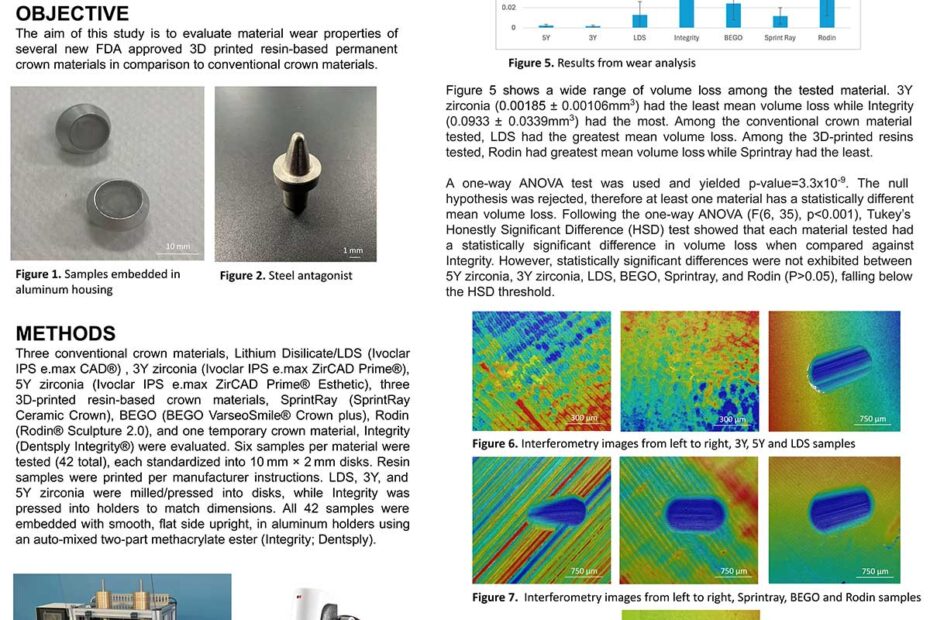
Evaluating Wear Properties of 3D Printed Crown Materials in Comparison to Conventional Crown Materials