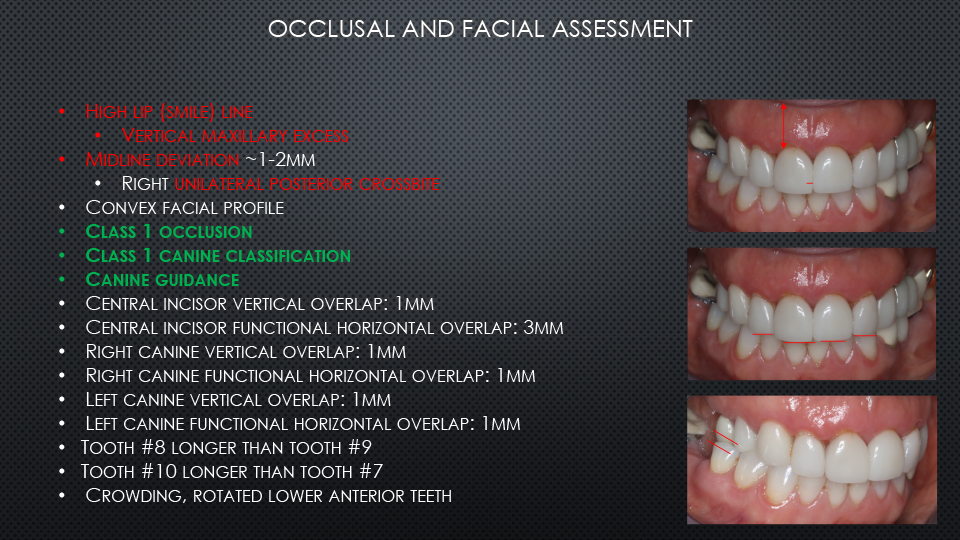
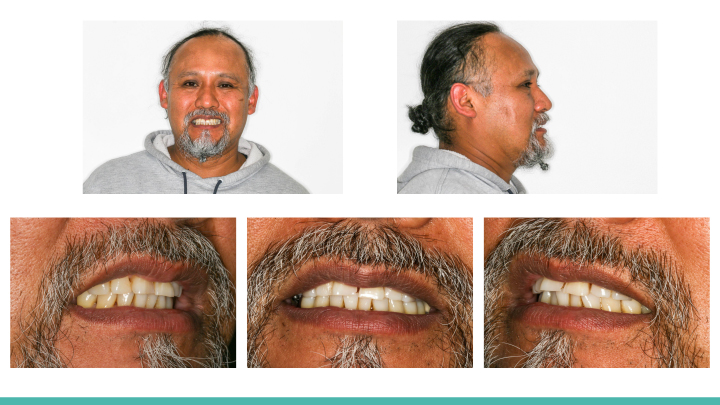
Aesthetic & Functional Oral Rehabilitation: A Multi-Disciplinary Case involving Periodontics, Orthodontics, Implants, Veneers, and Crowns
Oral Rehabilitation with Immediate Dentures for a Patient Presenting with Drug-Induced Gingival Hyperplasia