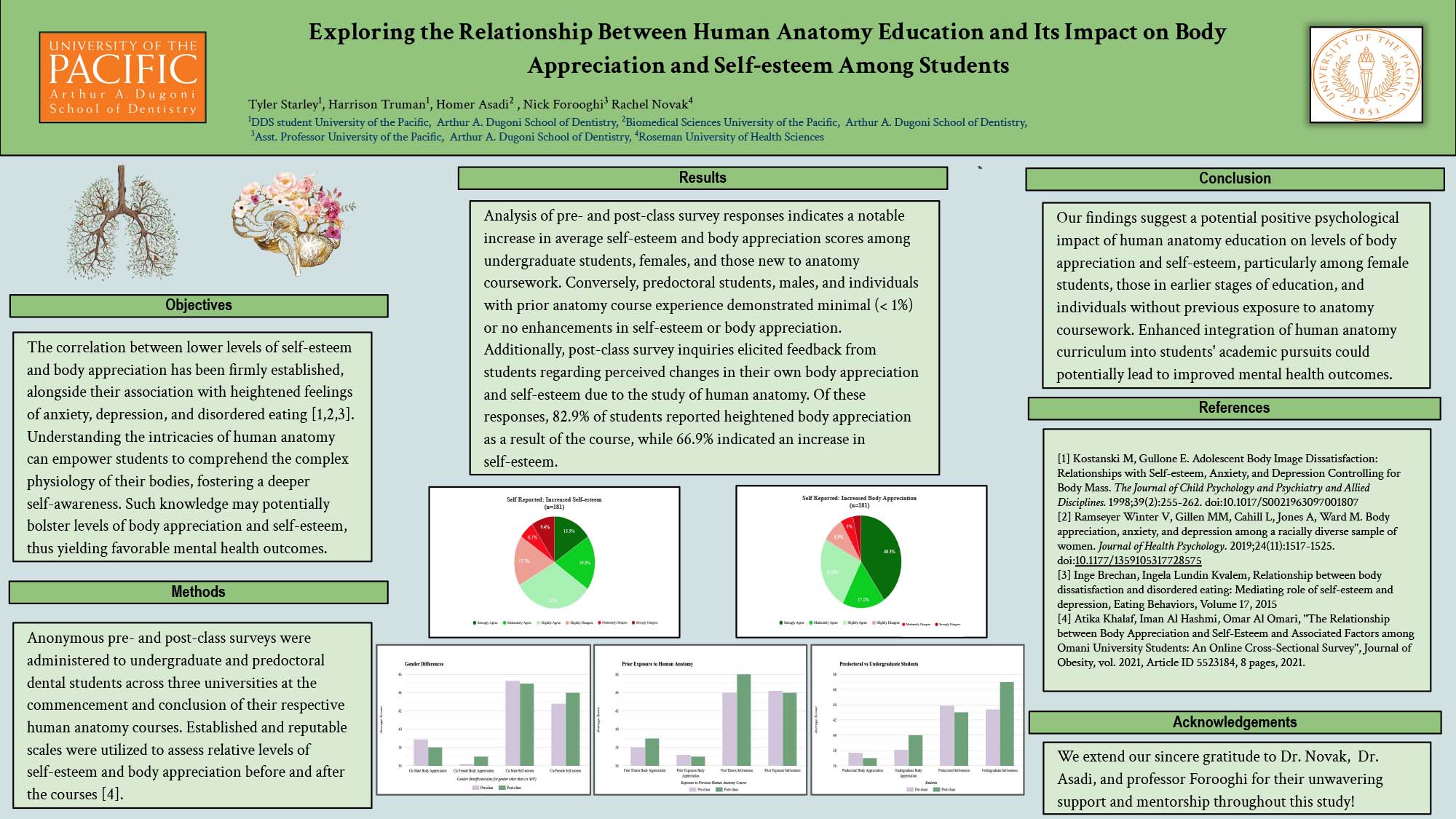
Exploring the Relationship Between Human Anatomy Education and Its Impact on Body Appreciation and Self-esteem Among Students
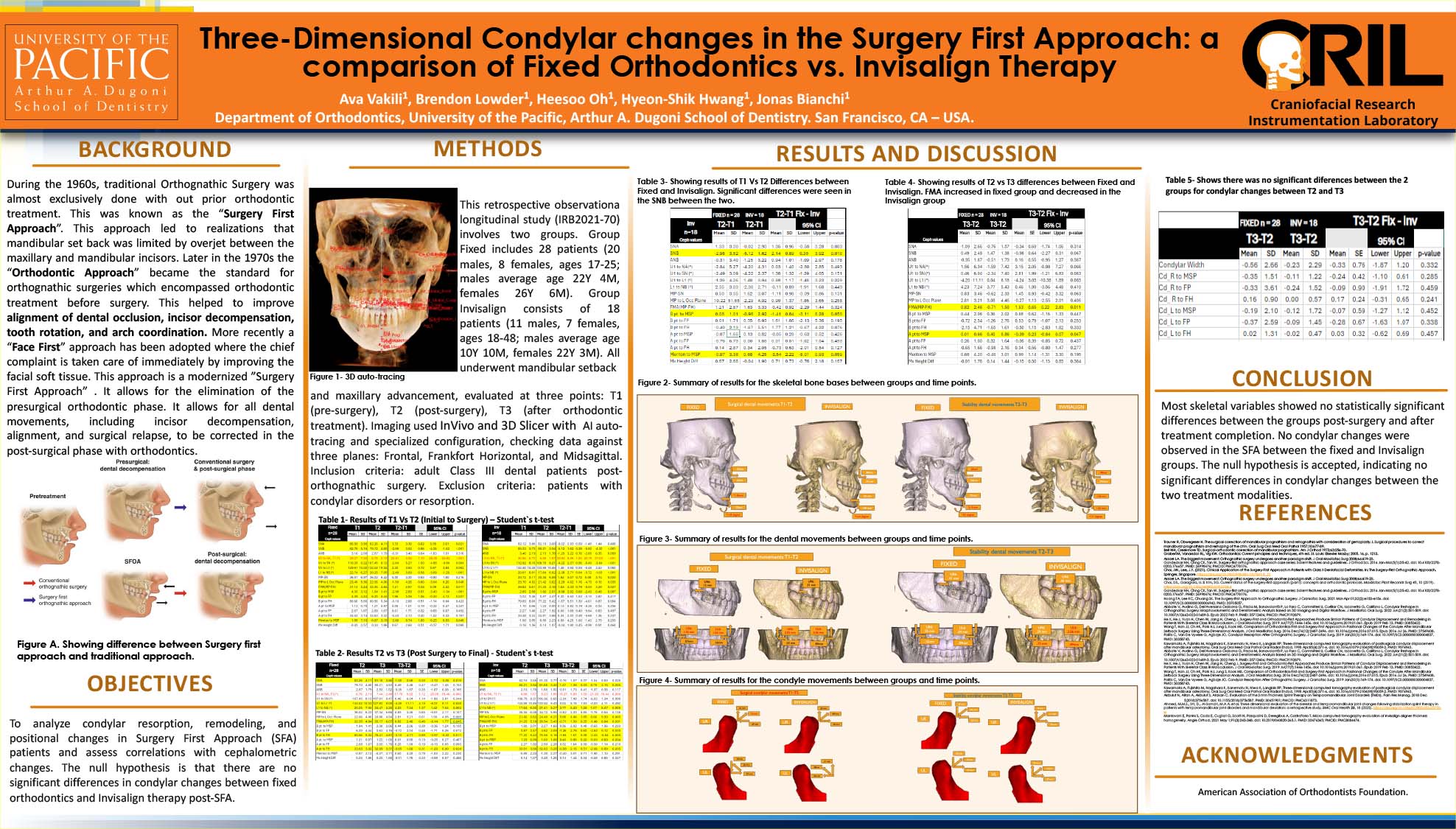
Three-Dimensional Condylar Changes in the Surgery First Approach: A Comparison of Fixed Orthodontics vs. Invisalign Therapy
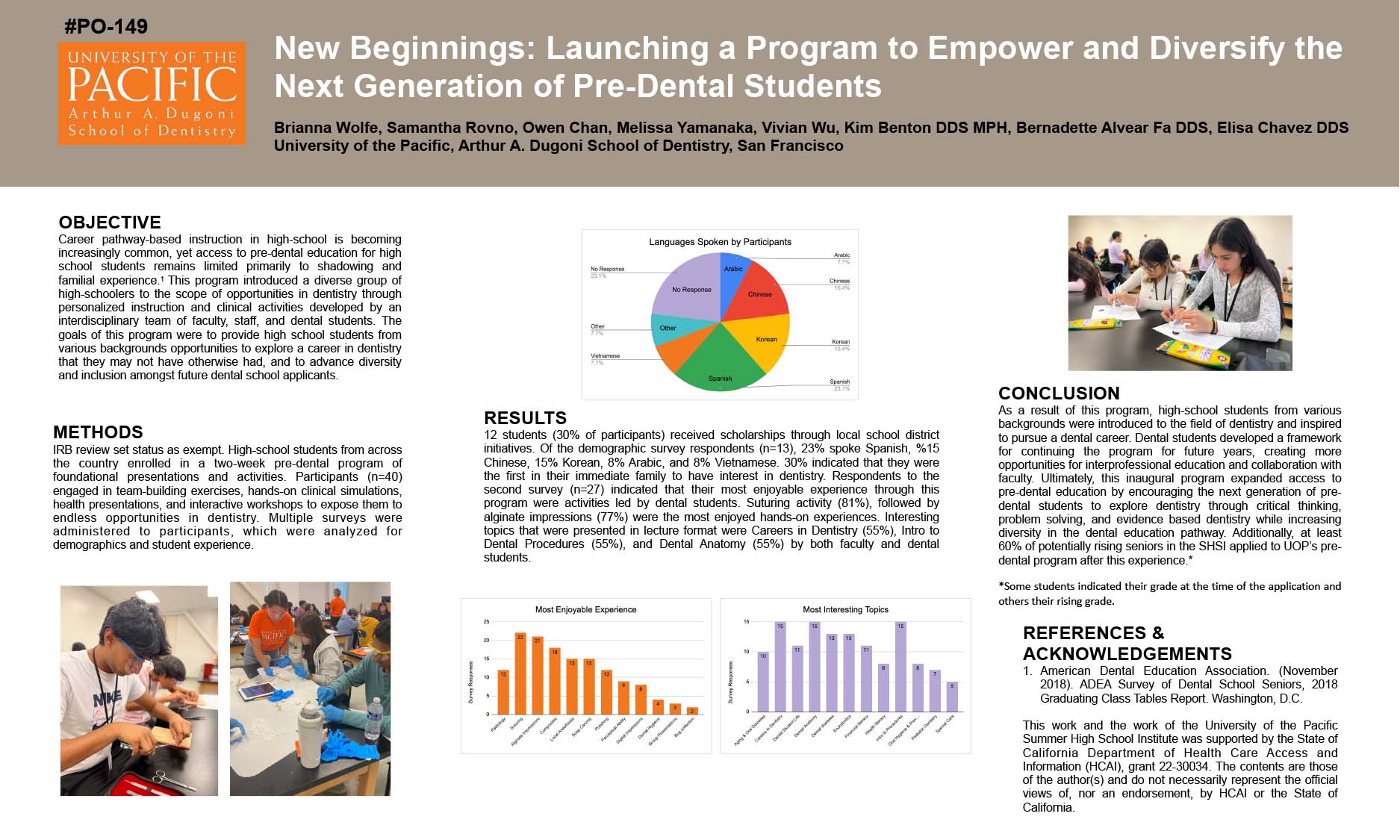
New Beginnings: Launching a Program to Empower and Diversify the Next Generation of Pre-Dental Students
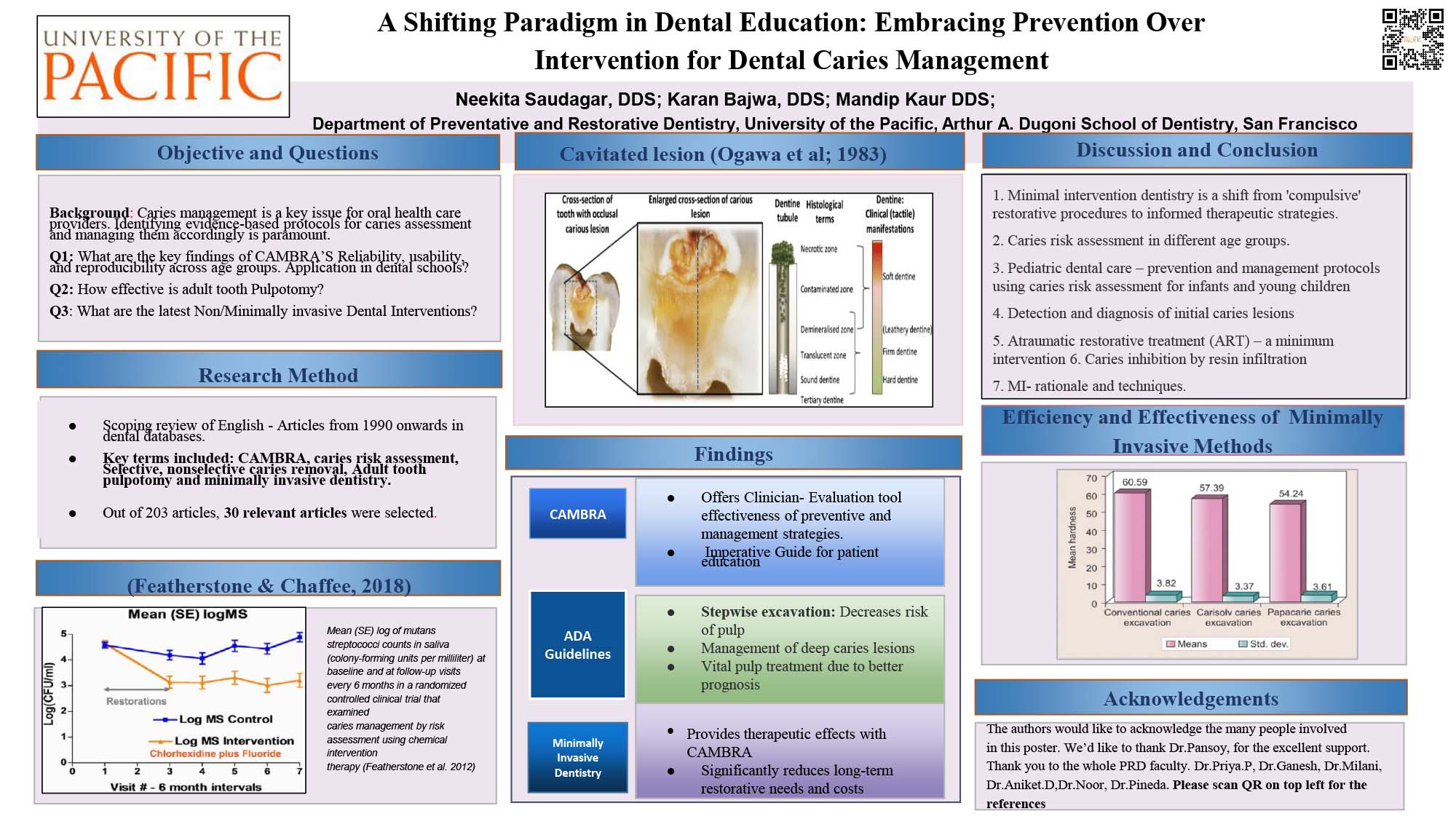
A Shifting Paradigm in Dental Education: Embracing Prevention Over Intervention for Dental Caries Management