Restoration of Oral Function in Severe Tooth Erosion Arising from Gastroesophageal Reflux Disease (GERD): A Clinical Case Study
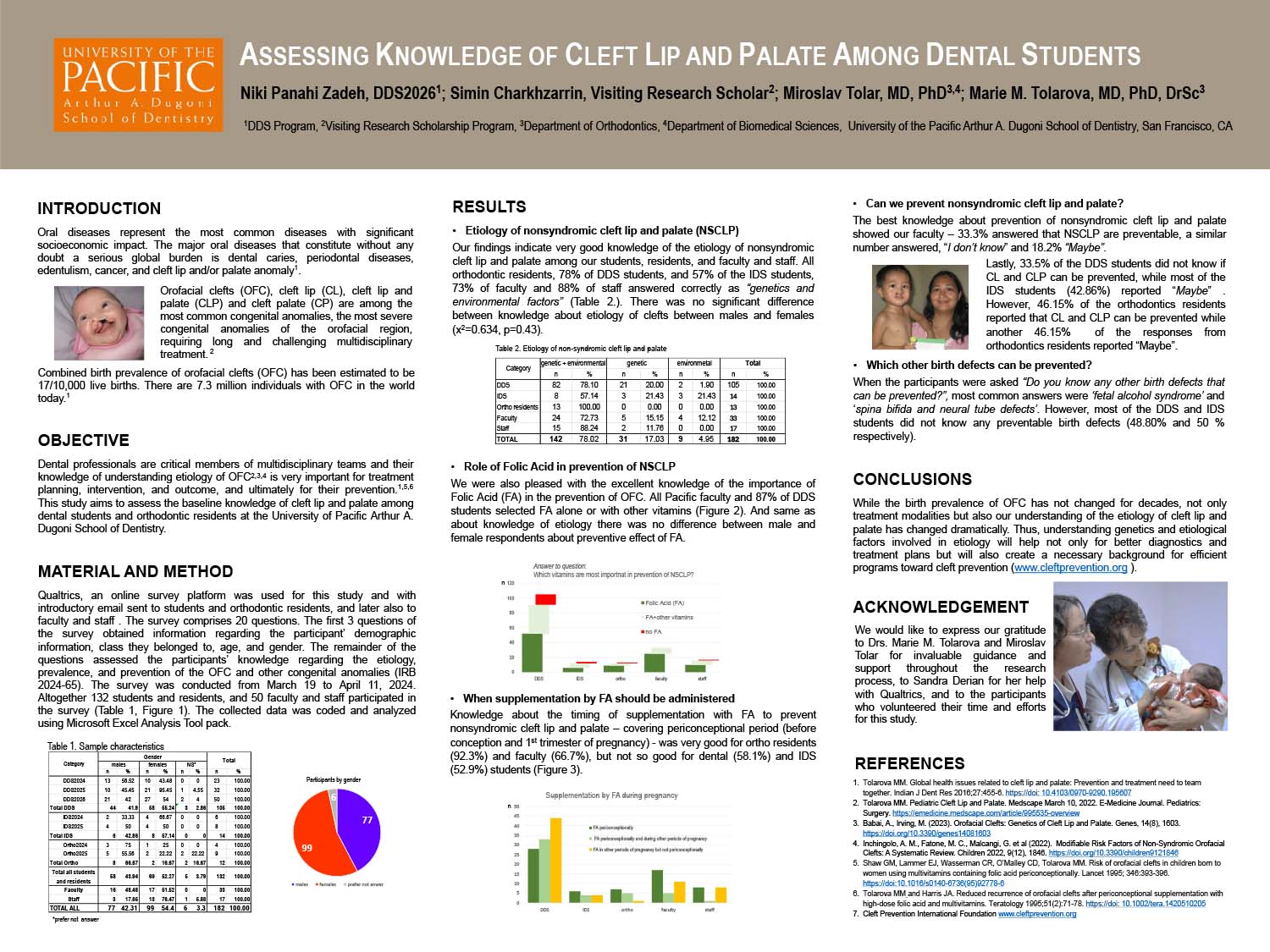
Assessing Knowledge of Cleft Lip and Palate Among Dental Students at the University of Pacific Arthur A. Dugoni School of Dentistry
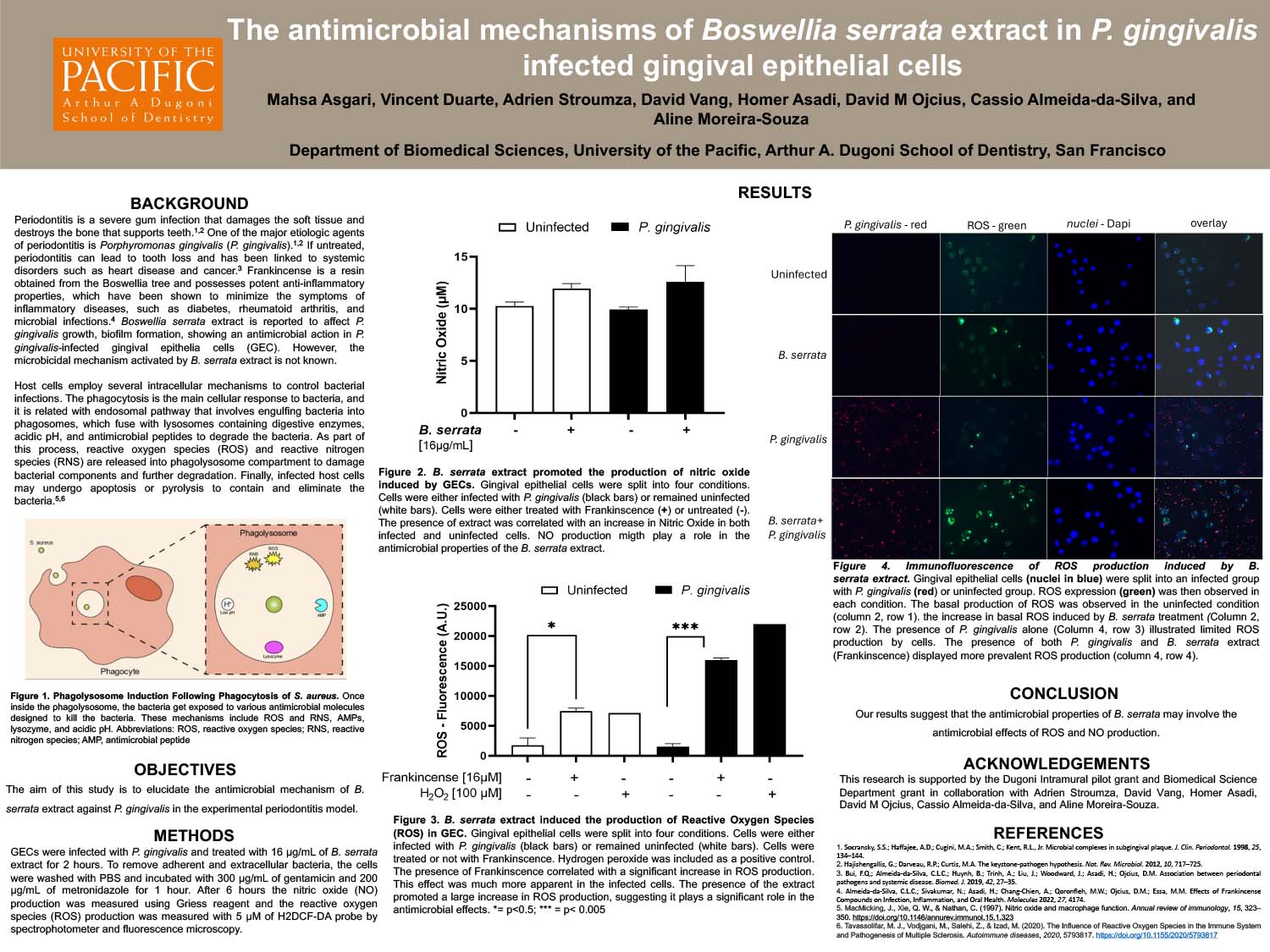
The Antimicrobial Mechanisms of Boswellia serrata extract in P. gingivalis infected gingival epithelial cells